75 yr old male came to opd with chief complaints of
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
A 75yr old male from nalgonda came to opd with,
CHIEF COMPLAINTS: pain in abdomen since 4 months
bilateral knee pain since 20yrs
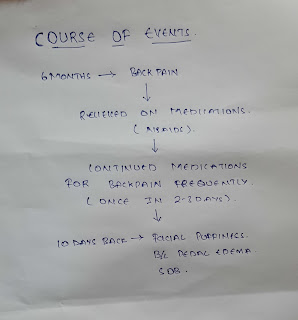
HISTORY OF PRESENTING ILLNESS:patient was apparently asymptomatic 20 yrs back then he developed unilateral knee pain which was insidious in onset gradually progressive to both limbs,throbbing type pain.
Patient is unable to stand from sitting position or sit from standing position,walking with support since 5 to 6 yrs
No pain on rest aggrevated on standing and walking
History of pain around umbilicus region,gradually progressive insidious in onset ,burning type, aggrevated after eating spicy food since 4 months after 1 hr of eating food ,resolves spontaneously after 2 hrs
No history of weight loss or weight gain,nausea,vomiting,constipation,diarrhoea,
No history of headache,dizziness,burning micturition,malena.
. HISTORY OF PAST ILLNESS:
. K/c/o diabetes type 2 since 2 yrs not on medication
. Not a k/c/o HTN,CVA,CAD,TB,ASTHMA
. TREATMENT HISTORY:insignificant.
. PERSONAL HISTORY: His daily routine 20 years ago was he use to wake up at 6am in the morning and have tea and he use to look after his agriculture land and at 9a.m he use to have breakfast and continued his work till lunch at 2 o'clock then he use to rest for a while and continued his work till dinner time at 8 pm
After 8 he used to spend some time with family before going to sleep at 10 clock.
But due to unbearable knee pains he stopped working since 10 yrs.
He smoke 1 pack of beedi since 40 yrs
Dietary history
Breakfast - 4 idli or 1Dosa
Lunch - rice with Dal,vegetables and curd
Evening snacks- tea and biscuits
Dinner- chapathi with vegetable curry
Mixed diet
Appetite normal
Sleep adequate.
. FAMILY HISTORY:
. No significant family history
. GENERAL EXAMINATION :
,
. Patient was conscious coherent co-operative
Pallor - no
No icterus, cyanosis, clubbing, lymphadenopathy, edema.
VITALS
BP- 100/70mmhg
Bp - 90/60mmhg
PR -68 bpm
RR-22cpm
Spo2 98% at room air
Temperature - afebrile





System examination
ABDOMEN :
INSPECTION:
Shape – scaphoid
Flanks – free ,Umbilicus – central, Shape-inverted
Skin – no scars
Dilated veins – absent
PALPATION:
Superficial palpation-no tenderness
Deep palpation:
Liver:not palpable
Spleen:not palpable
Kidney: not palpable
PERCUSSION : Tympanic note heard all over the abdomen.
AUSCULTATION:
Bowel.sounds heard.
CVS: S1 S2 heard , jvp not raised,apex beat pounding , heart sounds normal,no murmurs
RS: BAE present ,NVBS heard.
Trachea central
Chest movements normal
CNS: NFND,higher mental functions normal.
. LOCAL EXAMINATION OF KNEE:
No crepitus
Flexion deformities present.
Movements restricted on extension.
No swelling
No tenderness
No redness
Provisional diagnosis: non ulcer dyspepsia
Bilateral.osteoarthtitis.
Investigations:


TREATMENT:
TAB RAZO D 40 MG PO/OD 7AM
TAB ULTRACET 1/2 TAB QID
SUP. ALKASTON B6 PO/BD,10ML IN ONE GLASS OF WATER.
.

Comments
Post a Comment